Obesity and Overweight Trends for Children in America

About 1 in 3 children and teens ages 6 to 17 in the United States are living with obesity or overweight, according to 2022–23 data on the KIDS COUNT Data Center. While this figure has hovered around 32% to 34% in recent years, it has grown considerably over the last several decades. Being overweight or obese affects young people’s physical and emotional health in the short-term and often has lasting health risks into adulthood. For example, kids who struggle with their weight face higher risks of diabetes, heart disease and other chronic conditions as they age. Childhood obesity and overweight in America are deeply connected to the environments in which young people live, learn and play — including access to nutritious and affordable foods, safe opportunities for physical activity, quality health care and family resources.
This post explores what childhood obesity and overweight mean, why they develop and how rates differ across communities and demographic groups. Understanding these patterns is critical for policymakers, health professionals, educators and families working to support healthier futures for young people. By examining the causes and disparities surrounding obesity in children, we can better identify solutions that foster lasting well-being and reduce health inequities across the country.
What is Childhood Obesity or Overweight?
Childhood obesity and overweight are typically defined using a child’s Body Mass Index (BMI), a measurement that compares height and weight and adjusts for age and sex. Children with a BMI between the 85th and 95th percentiles are considered overweight, while those at or above the 95th percentile are considered obese. Severe obesity refers to a BMI that is significantly above the 95th percentile. This approach to defining these conditions allows health providers to account for children’s natural growth patterns, which change as they get older.
Researchers and clinicians track BMI trends over time to understand how rates are shifting across communities and demographic groups. Because BMI alone does not capture every aspect of health, many health experts pair BMI data with other measures, such as metabolism, and information about nutrition, physical activity, family history and social conditions. Together, this provides a clearer picture of children’s health and helps identify where additional support and resources may be most needed.
It is important to acknowledge that BMI is based on non-Hispanic white body types and it does not take into account race or ethnicity. Being a larger size does not necessarily mean one is unhealthy, and labeling children as overweight or obese can be stigmatizing and harmful. The AMA has adopted a policy addressing the limitations of the BMI, and efforts are under way to improve measures of obesity and overweight.
Read more about the medical field’s evolving views on childhood obesity
What Factors Cause Childhood Obesity and Overweight?
There is no single cause of childhood obesity and overweight in America. Experts no longer focus narrowly on individual behaviors like diet and physical activity but, instead, describe this as a chronic health condition and point to a combination of socioeconomic,
Below are some of the key influences that researchers and pediatricians identify as contributing factors for childhood obesity and overweight:
- Nutrition and Food Access: Families may not always have access to fresh, affordable foods, particularly in neighborhoods where grocery stores are limited and fast-food options are more common. These barriers can shape health and habits over time. Additionally, the quality of food available in child care facilities and schools can influence children’s weight. AAP, RWJF and others talk about the importance of food environments in child care, school settings, etc.
- Physical Activity Opportunities: Safe play spaces, parks, recreation centers and school-based physical education all support active lifestyles. When these resources are limited or inaccessible, children may have fewer opportunities to be active.
- Family Income and Household Resources: Financial strain can affect meal planning, food access and choices, time available for physical activity and the ability to obtain quality health care. Families experiencing economic instability may face additional stress that influences health and wellness.
- Social and Emotional Well-Being: Stress, trauma, depression and other emotional challenges are strongly linked to unhealthy weight. Depression and childhood obesity, in particular, frequently occur together. Supporting mental health — along with sleep and screen use — is often an important component of addressing obesity and overweight in kids and teens.
- Genetics and Medical Conditions: Family history, biology and certain medical conditions can increase a child’s likelihood of gaining weight. While these factors play a role in what is considered a chronic disease, childhood obesity is typically understood alongside a host of broader socioeconomic, community and structural influences.
Together, these contributing factors reflect the broader systems and environments that shape daily life for young people and their families. Leaders can address the conditions and risk factors that lead to weight challenges for kids. Preventing and reducing childhood obesity effectively requires coordinated efforts across health care, education, community organizations and public policy — with a focus on equity and access to healthy opportunities.
National and State-Level Trends of Childhood Obesity
Childhood obesity rates in the U.S. have remained high in recent years. National survey data show that about 1 in 3 children and adolescents ages 6 to 17 are living with obesity or overweight — a level that has persisted in recent years and, for some states, continues to rise. These childhood obesity and overweight statistics in America underscore growing concerns among pediatricians, public health leaders and community organizations working to support the health and well-being of young people.
Rates of obesity or overweight among young people vary across the country and are influenced by differences in local economic conditions, policies, infrastructure, household income and access to food and community resources. For example, children living in Southern areas of the country tend to have higher rates of obesity or overweight compared to those in other regions, reflecting these types of differences. In 2022–23, 20 states and D.C. exceeded the national rate (32%) of obese or overweight children — more than half of these states were located in the Southern region of the nation (see map below). In three states, at least 2 in 5 kids were struggling with obesity or overweight, the highest shares in the country: Mississippi (43% in 2022–23), West Virginia (41%) and Arkansas (40%).
State map of children and teens overweight or obese, 2022–2023
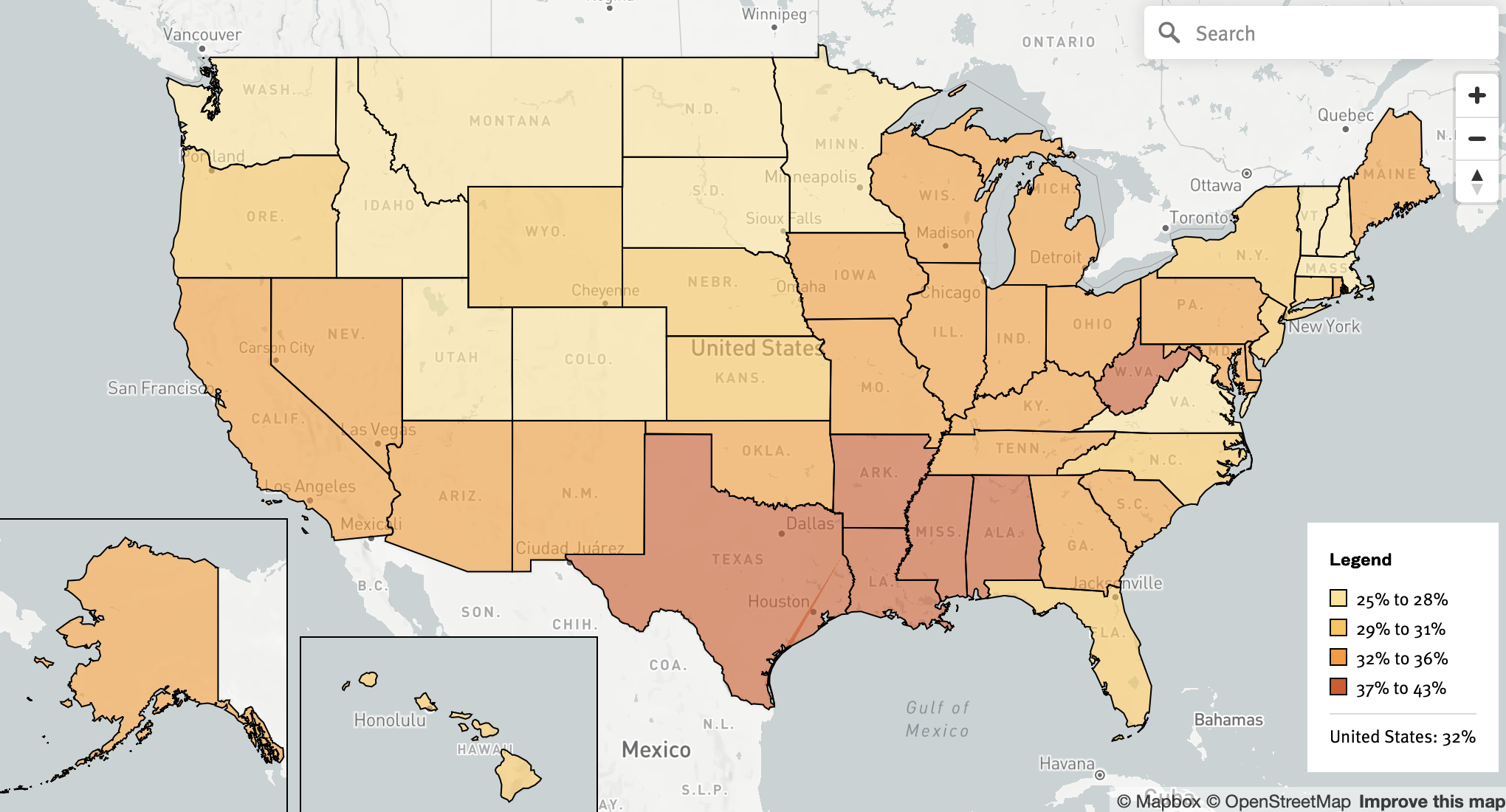
About half of the states including D.C. saw their rates of childhood obesity or overweight worsen from 2016–17 (the earliest year available on the KIDS COUNT Data Center) to 2022–23, with three states experiencing jumps of 6 percentage points: Arkansas, Alaska and Arizona.
Inequities in Childhood Obesity and Overweight by Demographic Group
Rates of obesity and overweight differ substantially by racial and ethnic group in America. These disparate outcomes have persisted for decades, as underlying social determinants of health (such as those outlined above) play a key role in these chronic health conditions. The 2025 KIDS COUNT Data Book reported, for instance, the following inequities for youth ages 10 to 17 who were obese or overweight in 2022–23:
- Latino: 39%
- Black: 38%
- American Indian or Alaska Native: 34%
- Multiracial: 30%
- White: 26%
- Asian and Pacific Islander: 22%
Additional groups of young people face elevated risks of obesity, as well. These include but are not limited to children and youth who:
- Live in families with low incomes or low parental education levels, partly because they may have less access to nutritious food and physical activity opportunities.
- Live with disabilities or special health care needs.
- Have had two or more adverse childhood events, which are potentially traumatic experiences that can threaten a child’s physical and mental health, such as family violence, abuse or loss of a parent.
Also see child and teen obesity or overweight statistics in America by gender
Understanding rates of childhood obesity or overweight in the U.S. — and how they differ across states and demographic groups — helps policymakers and local leaders identify where targeted supports are most needed. These data can guide investments to improve nutrition programs, physical activity opportunities, family resource centers and other strategies that promote healthy growth for all children.
Ultimately, reducing the child and teen obesity or overweight rate in America will require leaders at all levels and in multiple sectors to employ comprehensive and equitable approaches to prevention, health promotion and access to care for families.


